
1. Plain English Summary
2. Background and Unmet Need
Individuals with severe, long-term peripheral vascular damage frequently present with Difficult Venous Access (DVA), requiring multiple, highly distressed insertion attempts spanning extended periods. In traditional disposable syringes, an initial failed attempt introduces blood directly into the primary fluid barrel, where it rapidly mixes with and obscures the active therapeutic payload, completely darkening the solution.
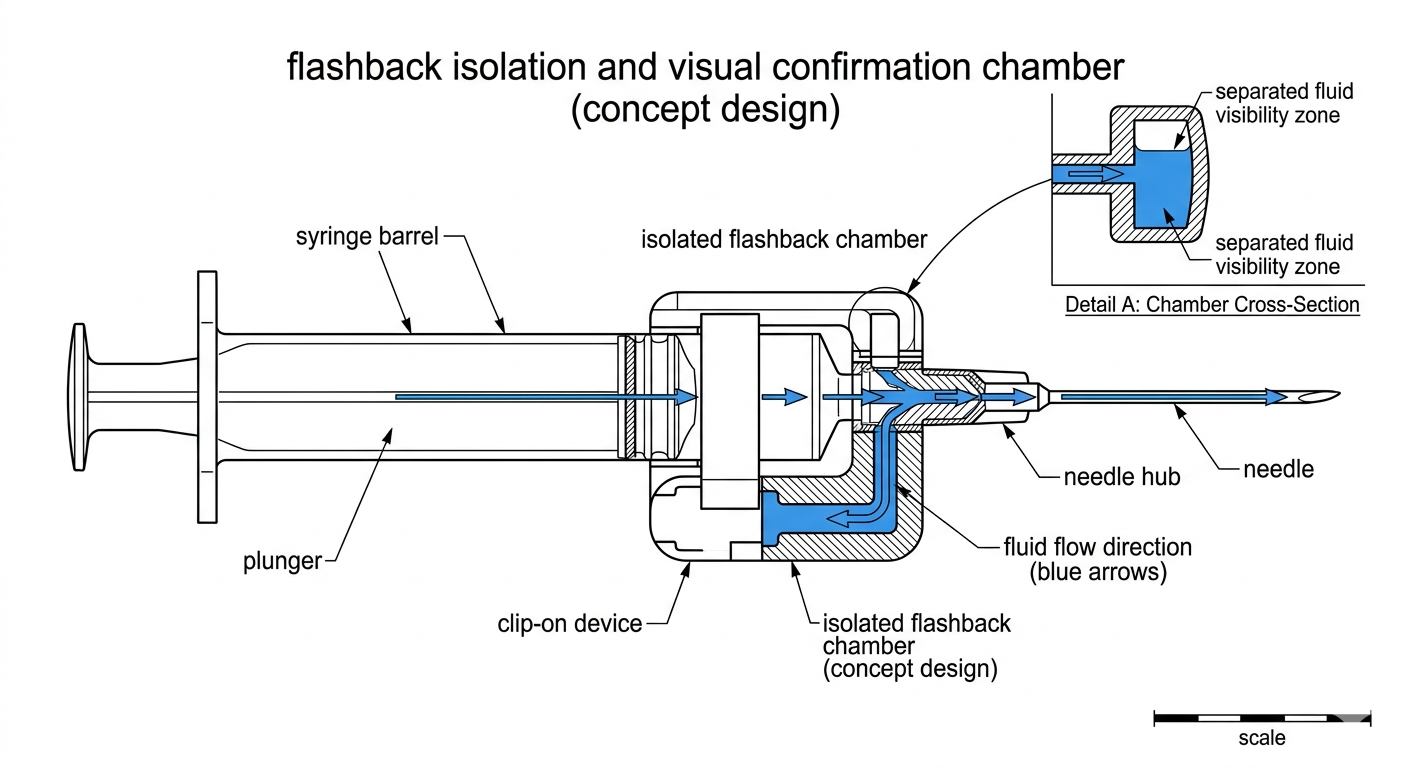
Crucially, during extended or recursive placement attempts, this misplaced blood rapidly congeals inside the primary barrel, jamming the plunger mechanism and ruining the payload. Facing a failing mechanical system and total loss of visual feedback, service users are frequently forced into highly hazardous blind tissue tracking. Because standard syringe barrels are transparent, a mere "visibility window" offers no structural benefit; instead, there is an urgent public health requirement for a low-cost, in-line Luer-lock adjunct asset that mounts directly between the barrel and needle hub to physically trap and isolate flashback fluid, completely preventing coagulation inside the primary payload barrel.
3. Research Question
4. Work Packages
WP1 – Engineering, Fluid Dynamics & Luer-Lock Interface Optimization
Mechanical optimization of the in-line Luer-lock connection tolerances, internal valve/fluid-gate separation stability, and secure fluid routing metrics across standard NHS/NSP syringe and needle hub brands.
WP2 – Human Factors & Multi-Attempt Usability Testing
Simulated human-factors evaluation measuring chamber containment efficacy and user interpretation during recursive, extended-time vascular access scenarios with clinical and outreach stakeholders.
WP3 – Contamination & Safety Risk Assessment
Rigorous hazard identification focusing on fluid retention boundaries, physical Luer-lock attachment stability under pressure, and cross-contamination mitigation profiles.
WP4 – Feasibility Pilot
Small-scale observational evaluation of the in-line Luer-lock adjunct within established community harm reduction networks (subject to full ethics and MHRA approval).
WP5 – Analysis & Health Economics Dissemination
Evaluation of success metrics, soft-tissue complication reduction data, and regional supply chain integration planning for full NIHR clinical scaling.
5. Cost Breakdown (Indicative NIHR Feasibility Budget)
| Category | Description | Estimated Cost (£) |
|---|---|---|
| Prototype Development & Engineering | Medical-grade polymer selection, high-tolerance in-line Luer hub fabrication, and fluid-gate testing | £22,000 |
| Human Factors Testing | Simulation lab hire, clinician/outreach staff participation, and usability evaluation | £25,000 |
| PPIE Engagement | Compulsory service user involvement sessions, peer-advocate compensation, and co-design workshops | £8,000 |
| Regulatory & Safety Review | Specialist medical device consultant fees for MHRA/UKCA adjunct device pipeline classification | £18,000 |
| Project Management & Analysis | Ethics clearances, data analysis, health economics reporting, and clinical scaling coordination | £25,000 |
| Total Estimated Budget | £98,000 | |
6. Outcome Measures
- Complete isolation of initial blood flashback into the intermediate Luer chamber
- Prevention of blood mixing, clouding, and congealing inside the main payload barrel
- Measurable reduction in blind tissue tracking and procedural access duration
- Validated System Usability Scale (SUS) performance scores among frontline needle exchange networks
7. Equality, Diversity & Inclusion
Explicitly tailored to address severe health inequities within historically underserved, highly marginalized populations interacting with community harm reduction assets, ensuring direct peer-led evaluation across diverse regional deployment settings.
8. Risk Register
Chief Investigator / Applicant
Mark Gomersall
markgomersall2@gmail.com